Electrodiagnostic studies are useful diagnostic tools for localizing and characterizing pathology in nerve or muscle. Among the conditions amenable to electrodiagnostic evaluation are focal neuropathies, radiculopathies, or plexopathies; polyneuropathies; and other neuromuscular lesions (eg, myopathies and central lesions). Information rendered by electrodiagnostic studies includes the type of pathology, its location, and its severity.
A thorough history and physical examination is the prerequisite to an accurate electrodiagnostic workup. Particular attention must be placed on recognizing patterns of weakness, sensory abnormalities, or pain. Patterns that must be observed include location (proximal versus distal or symmetric versus asymmetric involvement) and type (motor versus sensory). In this sense, electrodiagnostic testing is an extension of the history and physical examination, and the results must be interpreted in the context of the foundation established by the clinical data.
It is not the intention of this chapter to empower the reader to successfully interpret the raw data of electrodiagnostic studies; rather, it is to provide an appreciation of what these studies can reveal and to introduce and review the basic science that underlies the observed responses.
A complete electrodiagnostic evaluation consists of nerve conduction studies (NCSs) (also known as nerve conduction velocity tests) and electromyography (EMG). Each part of the evaluation offers distinct information. Unless there are specific contraindications, a complete electrodiagnostic study should include both NCSs and EMG. The combined testing is commonly referred to as EMG.
Nerve Conduction Studies
Nerve conduction studies test the speed by which motor, sensory, or mixed (combined motor and sensory) nerves transmit impulses. The nerves most often studied are the median, ulnar, and radial nerves in the arm and the tibial, peroneal, and sural nerves in the leg. In this noninvasive and essentially painless test, two pairs of surface electrodes are placed on the skin: one pair proximal and one pair more distal. The general format is as follows: the proximal pair stimulates the nerve with a very mild electrical impulse, and the distal pair records the resulting electrical activity. The time it takes for electrical impulses to travel between the electrodes is noted; this value is then divided by the known distance between the electrodes to yield the nerve conduction velocity.
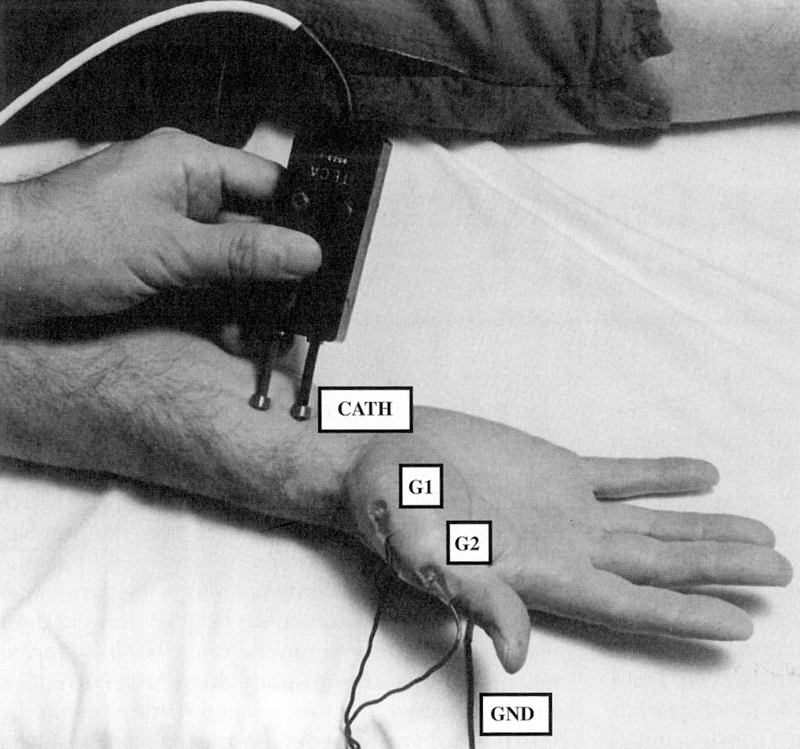
Motor nerve conduction studies are performed by placing recording electrodes over a muscle and stimulating the nerve that innervates that muscle (Fig. 1

Figure 1 Motor nerve conduction study setup. The active recording electrode (G1) is placed on the center of the muscle, and the reference electrode (G2) is placed distally over the tendon. CATH = stimulator cathode, GND = ground.
(Reproduced with permission from Preston DC, Shapiro BE: Electromyography and Neuromuscular Disorders: Clinical-Electrophysiologic Correlations. Boston, MA, Butterworth-Heinemann, 1998, p 26.)
). The recording electrodes consist of an active electrode placed over the muscle and a reference electrode placed distally over its tendon. The nerve innervating the muscle is then stimulated, usually at a proximal and distal site. The response recorded over the muscle is called a compound muscle action potential(CMAP). The CMAP can be described in terms of latency, amplitude, and conduction velocity (Fig. 2

Figure 2 Compound muscle action potential (CMAP). Latency measures the delay between stimulus and response.
(Reproduced with permission from Preston DC, Shapiro BE: Electromyography and Neuromuscular Disorders: Clinical-Electrophysiologic Correlations. Boston, MA, Butterworth-Heinemann, 1998, p 27.)
). Latency denotes the time required to note the initial response of the muscle after the application of the stimulus. Amplitude reflects the magnitude of the response and is proportional to the total number of nerve fibers activated.
If the appearance of the CMAP is considered to be the “response” to stimulation, the conduction velocity cannot be calculated unless the nerve is stimulated at both a proximal and distal site. With such dual stimulation, the time required for the impulse to cross the neuromuscular junction (NMJ) and depolarize the muscle can be subtracted, yielding the nerve conduction time alone.
Sensory nerve conduction studies are performed by placing a recording and reference electrode over the nerve to be examined and then stimulating the nerve proximal or distal to the recording site (Fig. 3

Figure 3 Sensory nerve conduction study setup. Ring electrodes are placed over the index finger, 3 to 4 cm apart. The active recording electrode (G1) is placed more proximally, closest to the stimulator. CATH = stimulator cathode, GND = ground, G2 = reference electrode.
(Reproduced with permission from Preston DC, Shapiro BE: Electromyography and Neuromuscular Disorders: Clinical-Electrophysiologic Correlations. Boston, MA, Butterworth-Heinemann, 1998, p 29.)
). The response is called a sensory nerve action potential(SNAP) and, as with CMAP, is quantified by latency, amplitude, and conduction velocity (Fig. 4

Figure 4 Sensory nerve action potential (SNAP). Onset latency measures the interval between the stimulus and the onset of response; peak latency measures the interval between stimulus and maximal repsonse.
(Reproduced with permission from Preston DC, Shapiro BE: Electromyography and Neuromuscular Disorders: Clinical-Electrophysiologic Correlations. Boston, MA, Butterworth-Heinemann, 1998, p 30.)
). Because the SNAP is stimulated and recorded over the nerve, no NMJ or muscle depolarization time has to be accounted for, and conduction velocity can be calculated with one stimulation site.
NCSs also can be used to assess F waves in addition to the CMAP response. F waves represent delayed muscular stimulation that occurs after and as a result of the initial motor nerve stimulation. F waves appear as a “backfiring” or echo—the very same nerve impulse that leads to muscle contraction also travels away from the muscle toward the spinal cord, where it can stimulate the motor neuron in the spinal cord. This sends a recurrent antegrade nerve impulse that results in a second, delayed motor response. F-wave measurements reflect conduction along the entire nerve and are useful in the study of general polyneuropathies and Guillain-Barré syndrome.
As the F wave is routinely measured from a distal muscle, the latency may be prolonged in distal entrapments as well as in diseases of the proximal neuron. It may be more useful to think of the F wave as a nonspecific test of the entire nerve circuit.
Electromyography
Electromyography (EMG) is a test that measures the electrical response of muscle contraction; in this respect, it is similar to an electrocardiogram, which is a test that measures the electrical effects of heart muscle contraction. EMG (or needle electromyographic examination) involves inserting a needle into a muscle and evaluating spontaneous and voluntary activity as detected by an electrode (Fig. 5

Figure 5 During EMG, a needle electrode is inserted into the muscle. The oscilloscope (not shown) registers the shape, size, and presence of the waveform of the action potential of each contracting muscle fiber, providing data regarding the muscle’s response to stimulation of the nerves more proximally (not shown).(© A.D.A.M., Inc.)
). This test is considered by many to be mildly uncomfortable and is, by its nature, invasive.
EMG is an integral part of the electrodiagnostic study. Abnormal activity may be seen in disease states ranging from motor neuron disease to myopathy. EMG is very important in determining not only the severity of pathology but also the chronicity. It can be used for evaluating proximal muscles that are not easily studied with NCSs and often yields important information about the nervous system. It can be helpful, for example, in differentiating between primary nerve and muscle dysfunction and partial and complete nerve dysfunction.
After the resolution of the insertional activity (electrical activity in the muscle elicited by mechanical stimulation), there should be a period of electrical silence. A normal muscle will have no activity at rest. Common findings in acute denervation include fibrillation potentials (Fig. 6

Figure 6 Fibrillation potential. Spontaneous depolarization of a single muscle fiber. This pattern may indicate acute denervation.
(Reproduced with permission from Preston DC, Shapiro BE: Electromyography and Neuromuscular Disorders: Clinical-Electrophysiologic Correlations. Boston, MA, Butterworth-Heinemann, 1998, p 184.)
) or positive sharp waves, which represent the spontaneous depolarization of a single muscle fiber. Fasciculations result from spontaneous activity of groups of muscle fibers. These are common in amyotrophic lateral sclerosis (ALS). This first part of the EMG can help differentiate between primary muscle disease and apparent muscle dysfunction caused by denervation; in the latter, the muscle may be seen to fire at rest.
Voluntary activity is then evaluated by asking the patient to contract the muscle being examined. Motor unit action potential (MUAP) morphology is evaluated for amplitude, duration, and the pattern of activation and recruitment of muscle fibers. In general, neuropathies with adequate time for reinnervation can demonstrate large amplitude, duration, and/or polyphasic MUAPs. Recruitment of MUAPs is decreased with axonal loss or with demyelination and conduction block.
Variables that affect NCS results are numerous and include temperature, age, height, anomalous innervations, and timing of the electrodiagnostic study relative to the onset of injury.The recognition of these variables and patterns is essential to avoid making mistakes in diagnosis. Cool temperatures slow conduction velocity, prolong latencies, and increase CMAP and SNAP amplitudes. Skin temperatures should be monitored and maintained, ideally, between 33°C (91.4°F) and 34°C (93.2°F) during the electrophysiologic examination. Conduction velocities and CMAP and SNAP amplitudes decrease with advancing age. Decreased nerve conduction velocities are seen in tall patients. Knowledge of anomalous innervations and their subsequent NCS patterns is also important to avoid mistaking a normal anatomic variant for nerve pathology.
Appreciation of the timing of the electrodiagnostic study relative to the time of the injury, if any, is very important because injured nerves undergo wallerian degeneration, a process that affects the nerve beyond the immediate location of injury. Wallerian degeneration is the means by which injured axons are broken down. It is characterized by Schwann cell degradation of the myelin sheath—a process that clears a path, so to speak, for the regenerating axons. The degeneration extends proximally from the injury to the preceding node of Ranvier and distally to the axon terminus. This process is not complete until approximately 7 days after injury.
Because of the timing of axonal degeneration, an NCS with stimulation and recording done distal to the lesion may produce normal results if performed too soon after injury; the distal axon functions normally. Conduction block (with demyelinating lesions) may be the only abnormality seen before wallerian degeneration occurs. EMG abnormalities occur in a proximal to distal temporal pattern. For example, in a proximal lesion (radiculopathy), the paraspinal muscles are affected first, and then more distal muscles are affected. Fibrillations or positive sharp waves obtained during EMG may take 1 to 2 weeks to occur in proximal muscles and 5 to 6 weeks to occur in more distal muscles. Reinnervated-appearing MUAPs (large amplitude, duration, or polyphasia) will also occur in a proximal to distal fashion, with early changes seen within 2 to 3 months after the injury. Knowledge of the acuity of the lesion and the time in which potential abnormalities may develop is essential to interpret results and recommend proper timing of the study.
Clinical Electrodiagnostic Testing
The purpose and scope of this section is not to extensively review all of the described neuromuscular disorders; rather, it is to provide an overview of commonly encountered disorders with a specific focus on their anatomy, presentation, examination findings, and related electrodiagnostic findings.
Motor Neuron Diseases
Motor neuron diseases are a group of disorders characterized by progressive deterioration of motor neurons. The most common form is ALS. This is a progressive disorder affecting both upper and lower motor neurons, usually beginning in a segmental distribution (ie, hand or leg), with symmetric or asymmetric involvement. Weakness, muscle wasting, and fasciculations are common findings on presentation. Speech and/or swallowing difficulties and respiratory compromise may occur. Physical examination findings include mixed upper and lower motor neuron signs, such as atrophy, hyperreflexia, and weakness. Sensation is spared.
Electrodiagnostic studies are useful in the workup of motor neuron diseases, but the diagnosis remains a clinical one. Electrodiagnostic studies can also be very useful to evaluate other potential diagnoses, such as spinal stenosis. NCSs should include motor and sensory studies in the upper and lower extremities of the affected side. Motor NCS results may be normal or have decreased CMAP amplitudes. Sensory NCS results are normal, but the presence of sensory abnormalities may suggest coexisting neuropathies and does not rule out motor neuron disease.
Radiculopathies
Electrodiagnostic evaluation is an important tool in combination with imaging studies in the evaluation of cervical and lumbar radiculopathies. These conditions are often caused by nerve root compression, disk impingement, or central or neuroforaminal stenosis. Imaging studies, such as MRI or CT, can demonstrate the structure of the nerve root and possible impingement, but these studies do not evaluate nerve function. Additionally, MRI has a substantial clinical false-positive rate; disk degeneration, herniation, and spondylosis are seen often in asymptomatic individuals.
Electrodiagnostic studies can be helpful to evaluate radiculopathy when imaging study results are normal and there is a high degree of clinical suspicion or when there are nonspecific abnormalities on the imaging study that do not correlate with the clinical presentation.
Electrodiagnostic studies can exclude more distal lesions, such as plexopathies, polyneuropathies, and mononeuropathies, and localize the level of involvement in multilevel degeneration or disease. For example, a patient who presents with thumb numbness, nocturnal paresthesias, neck pain, and cervical spondylosis may have a C6 radiculopathy, a median neuropathy at the wrist (carpal tunnel syndrome), or both. If MRI of the neck shows nonspecific mild to moderate multilevel disk degeneration with neuroforaminal stenosis, electrodiagnostic studies will be helpful to evaluate the presence or absence of a distal entrapment neuropathy or a coexisting cervical radiculopathy. Radiculopathies typically present with radiating arm or leg pain and are usually but not always associated with neck and back pain, paresthesias, or weakness.
Motor NCS results are usually normal in cases of radiculopathy but may show decreased CMAP amplitudes if there is significant axonal loss. Decreased CMAP amplitudes are less commonly seen in cervical radiculopathies. This is because the motor NCSs for the median and ulnar nerves are recorded over the muscles that are innervated by the C8 and T1 nerve roots (ie, the abductor pollicis brevis and abductor digiti minimi). These more caudal roots are less commonly involved in cervical radiculopathies.
As radiculopathies usually occur from compression of the nerve root proximal to the dorsal root ganglion, sensory NCS results are normal in these lesions. Therefore, sensory NCSs are very useful in localizing lesions proximal (radiculopathy) and distal (plexopathy, polyneuropathy, and mononeuropathy) to the dorsal root ganglion.
On EMG, abnormal spontaneous and voluntary activity can be seen in proximal and distal muscles of the affected extremity as well as the paraspinal muscles. The distribution of abnormalities should be in multiple peripheral nerves with a specific myotomal distribution. If muscles examined are limited to those innervated by a single nerve, a distinction cannot be made on the basis of EMG alone between a mononeuropathy and a radiculopathy. Paraspinal muscle involvement is very helpful in localizing the nerve lesion at or proximal to the nerve roots because the paraspinal muscles are innervated by the dorsal rami that arise directly from the spinal nerves.The absence of paraspinal involvement cannot, however, rule out a radiculopathy.
Plexopathies
The causes of brachial and lumbosacral plexopathies may be idiopathic, iatrogenic, traumatic, or neoplastic. Clinical findings on presentation include numbness and weakness with or without pain, depending on the etiology of the lesion. Weakness, altered sensation, and/or decreased reflexes in multiple peripheral nerve and nerve root distributions are also common. Electrodiagnostic testing can be very helpful in localizing and characterizing these complex lesions.
Routine motor NCSs may show decreased CMAP amplitude; conduction velocity may be decreased or normal, depending on the involved region of the plexus. Sensory NCSs are useful in localizing plexopathies because there are common sensory NCSs that can be performed to assess the C5 through T1 dermatomes. The results should be abnormal in plexopathies because the lesion is distal to the dorsal root ganglion. The distribution of abnormalities should be in the nerves supplied by the involved region of the plexus.
Polyneuropathies
Because etiologies of polyneuropathies are so numerous, electrodiagnostic evaluation is an important tool not only in establishing the diagnosis of polyneuropathy but also in characterizing specific polyneuropathies. Distinctions such as demyelinating or axonal and hereditary or acquired can help to narrow the differential diagnosis.
Polyneuropathies classically present as distal (stocking-glove) numbness and weakness. Pain may be present. On physical examination, a proximal to distal gradient of normal to abnormal symmetric findings is present. Polyneuropathies tend to appear distally first, with lower extremity involvement occurring before upper extremity involvement. Polyneuropathies usually affect both motor and sensory fibers, but there are predominately motor or sensory forms of polyneuropathies.
NCSs should be performed on both the upper and lower extremities. Motor and sensory NCS results will be abnormal, with more severe involvement in the lower extremities. Sensory NCS results may be more affected than motor NCS results. Limited comparison of the contralateral extremity will demonstrate symmetry of findings. If significant asymmetry is demonstrated, other diagnoses (such as plexopathy) should be considered. The presence of demyelination can be determined by the degree of latency prolongation and conduction velocity slowing. Conduction block may be present.
EMG should also show symmetric abnormalities in multiple peripheral nerve and nerve root distributions in a proximal to distal gradient. Lower extremity muscles should have greater involvement than upper extremity muscles. Proximal extremity or paraspinal muscles also should be examined; the presence of abnormalities in these muscles suggests more proximal pathology (ie, plexopathy and radiculopathy).
Mononeuropathies
An understanding of the anatomy of the upper and lower extremity will aid in identifying various mononeuropathies and differentiating these lesions from radiculopathies, plexopathies, polyneuropathies, and other lesions. As the electrodiagnostic studies are an extension of the physical examination, patterns of injuries will be similar, with abnormalities below the level of injury and normal function above the level of injury. Mononeuropathies of the upper extremities are commonly seen in the median, radial, and ulnar nerves and are often the result of direct compression.
The median nerve is the most commonly affected nerve in the arm, with the site of compression typically occurring at the carpal tunnel. Electrodiagnostic testing for carpal tunnel syndrome includes testing for median and ulnar motor and sensory responses. Specific comparison of the results of testing the median nerve with those of the ulnar nerve increases the electrodiagnostic sensitivity. Furthermore, two sequential comparison studies should be performed for patients with mild carpal tunnel syndrome to decrease the possibility of false-positive results in this population. EMG is performed to assess severity (axonal loss) as well as to exclude proximal median neuropathies, brachial plexopathies, and cervical radiculopathies.
Radial nerve compression can be a source of pain, weakness, and sensory disturbances. The radial nerve is commonly injured at the spiral groove of the humerus secondary to trauma or fracture. Radial neuropathies may occur in the axilla secondary to compression (as may be caused by using poorly fitting crutches, for example). When there is a radial nerve injury at the axilla, patients will have elbow extension (triceps) weakness. Sensory abnormalities may affect the posterior arm and forearm (posterior cutaneous nerve of arm and forearm). EMG can reveal triceps abnormalities; however, distinguishing a high radial neuropathy from a plexopathy (posterior cord) or radiculopathy requires evaluation of nonradial muscles (eg, deltoid and paraspinals). Furthermore, tests of the median and ulnar nerves and nonradial innervated muscles are performed to exclude radiculopathy, brachial plexopathy, or other possible lesions.
The posterior interosseous nerve (a branch of the radial nerve) can become entrapped near the elbow. Patients with such compression may have weakness on extension of the fingers and part of the wrist, but there should be no weakness proximal to the elbow. Sensation is preserved.
Ulnar neuropathies at the elbow are the second most commonly encountered nerve compression syndromes in the arm after carpal tunnel syndrome. It is more difficult to localize an ulnar neuropathy at the elbow than it is to localize a median neuropathy at the wrist using electrodiagnostic studies. Injuries of the lower trunk of the brachial plexus or the C8 and T1 nerve roots may also appear similar to an ulnar neuropathy, and electrodiagnostic studies will be helpful in localizing the injury. Entrapment of the ulnar nerve at the wrist occurs less commonly than at the elbow and may be associated with increased pressure over the ulnar surface of the palm, trauma, or compression.
Femoral neuropathies have been described in association with surgical procedures (eg, hysterectomy, hip arthroplasty, and renal transplantation) as well as with hyperextension injuries at the hip, tumors, diabetes mellitus, and iliopsoas hematomas. Depending on the etiology, patients may present with quadriceps weakness (knee buckling), decreased patellar reflexes, abnormal sensation or inguinal pain, swelling, or ecchymoses. A routine lower extremity electrodiagnostic examination will include testing of the tibial, peroneal, and sural nerves to differentiate plexopathies from polyneuropathies and saphenous and femoral motor studies to evaluate the femoral nerve. A screening examination of muscles innervated by the femoral, obturator, tibial, peroneal, and other nerves is performed to exclude a more generalized process.
Tibial nerve injuries are more common distally, where the nerve is more superficial. Proximal tibial neuropathies are described secondary to trauma (eg, penetrating injuries and knee dislocations), tumors, cysts, or entrapment at the soleus. Distally, the nerve can become compressed posterior to the medial malleolus, where it travels under the flexor retinaculum (tarsal tunnel syndrome). The clinical presentation may include paresthesias of the plantar foot, posterior calf numbness, plantar flexion weakness, abnormal Achilles reflexes, intrinsic foot muscle atrophy, and clawing of the toes. The differential diagnosis includes incomplete neuropathies, sacral plexopathies, and S1-2 radiculopathies.
The peroneal nerve is a continuation of the sciatic nerve, with motor and sensory fibers from the L4-S2 nerve roots. The nerve divides into superficial and deep branches posterolaterally below the knee. The superficial peroneal nerve provides motor branches to the peroneus longus and brevis muscles, as well as sensation to the dorsum of the foot. The deep peroneal nerve innervates the tibialis anterior, peroneus tertius, and toe extensor muscles and also provides sensation for the first web space on the dorsum of the foot. Injuries can occur at the common nerve or at either the deep or superficial branch.
The peroneal nerve can be injured by trauma (eg, knee injuries, ankle sprains, impact at the fibular head, and fractures), masses, compartment syndromes, entrapment, external compression, vascular compromise, and other conditions.
On physical examination, patients typically have dorsiflexion weakness (footdrop), eversion weakness (perceived as ankle instability), numbness, tenderness, and localized pain. The differential diagnosis includes L5 radiculopathies, lumbosacral plexopathies, sciatic neuropathies, and peripheral neuropathies.
Routine electrodiagnostic studies of the lower extremity include peroneal motor responses to the extensor digitorum brevis and are supplemented by peroneal motor studies to the tibialis anterior and superficial peroneal sensory responses. On EMG, both deep and superficial peroneal nerve innervated muscles are examined in addition to the short head of the biceps femoris, which is innervated by the common peroneal nerve. Muscles innervated by the tibial nerve are also examined, and more proximal muscles may need to be examined to differentiate a mononeuropathy from radiculopathies, plexopathies, and polyneuropathies, depending on the findings.
Neuromuscular Junction Disorders
Neuromuscular junction disorders are uncommon and usually present as symmetric proximal weakness and fatigue without sensory involvement that can be mistaken for myopathy. Eye findings, such as extraocular muscle weakness and ptosis, are common and may be asymmetric. Bulbar involvement may affect speech and swallowing. Physical examination findings usually include fatigability and proximal weakness, with preserved sensation and preserved reflexes. NMJ disorders can be classified by the site of dysfunction and include Lambert-Eaton myasthenic syndrome, tetanus and botulism (presynaptic), organophosphate poisoning (synaptic), and myasthenia gravis (postsynaptic). Routine electrodiagnostic testing is important to evaluate and rule out myopathies or other neuromuscular disorders with predominately motor involvement. Specialized electrodiagnostic testing using repetitive nerve stimulation can help make the diagnosis of an NMJ disorder and characterize the site of the pathophysiology.
Motor NCS results are usually normal in patients with myasthenia gravis; the CMAP amplitudes may be diffusely low in patients with Lambert-Eaton myasthenic syndrome. Sensory NCS results are usually normal, and there is usually no abnormal spontaneous activity on EMG, with the exception of botulism, which may have fibrillation potentials. Voluntary MUAPs may appear myopathic, with small amplitudes, short durations, and polyphasia. Repetitive nerve stimulation at a low frequency (3 Hz) can show a decreasing amplitude response in presynaptic and postsynaptic disorders. Repetitive nerve stimulation at a high frequency (50 Hz) will show an increasing amplitude response in presynaptic disorders.
Myopathies
Electrodiagnostic evaluation is a useful tool in combination with other diagnostic tests, such as muscle biopsy, to diagnose and characterize myopathic disorders. As with polyneuropathies, myopathies represent a wide and varied group of disorders that cannot be comprehensively covered within the scope of this chapter. Myopathies classically present with symmetric proximal weakness involving the upper extremities, lower extremities, or both. They may be acquired or hereditary, with weakness and functional impairments ranging from mild to severe. Sensation is not affected. Exceptions exist, and some myopathies may be asymmetric (eg, inclusion body myositis and facioscapulohumeral muscular dystrophy), distal (eg, myotonic dystrophy and inclusion body myositis), or painful (eg, dermatomyositis, polymyositis, and toxic myopathies). Physical examination findings include proximal weakness and atrophy, spared sensation, and usually normal reflexes.
Motor NCS results are usually normal because routine upper and lower extremity studies (ie, of the median, ulnar, tibial, and peroneal nerves) use recording electrodes over distal muscles, whereas myopathies typically affect proximal muscles. In severe myopathies or those with distal involvement, CMAP amplitudes may be low. Sensory NCS results will be normal. F waves are usually normal. NCSs are done to evaluate other disorders that may present with symptoms similar to those of myopathies (eg, motor neuron diseases, motor neuropathies, and NMJ disorders).
EMG is the most important part of the electrodiagnostic study in the workup of myopathy. Spontaneous activity may be absent or present and can help to narrow the differential diagnosis. Voluntary activity in myopathy is usually seen as small amplitude and duration, polyphasic MUAPs secondary to muscle fiber dysfunction, or dropout. However, this type of MUAP can be seen in a variety of disorders, including NMJ disorders, early reinnervation (nascent motor units), and periodic paralysis.
Recruitment is often described as “early” and can only be assessed by the examiner resisting the force generated by the patient during active muscle contraction. As the activated MUAPs have fewer muscle fibers, a smaller amount of force is generated than would typically be seen for the same amount of MUAPs being activated.
Key Terms
Compound muscle action potential (CMAP) The latency, amplitude, and conduction velocity recorded over muscle in motor nerve conduction studies
Electromyography (EMG) A test that measures the electrical response of muscle contraction
Mononeuropathies A group of disorders characterized by disease of a single nerve
Motor nerve conduction studies Studies that test the speed by which motor nerves transmit impulses by placing recording electrodes over a muscle and stimulating the nerve that innervates that muscle
Motor neuron diseases A group of disorders characterized by progressive deterioration of motor neurons
Myopathies A wide and varied group of primary muscle disorders characterized by weakness
Nerve conduction studies Studies that test the speed by which motor, sensory, or mixed (combined motor and sensory) nerves transmit impulses
Neuromuscular junction disorders A group of disorders affecting the neuromuscular junction characterized by symmetric proximal weakness without sensory involvement
Plexopathies A group of disorders characterized by numbness and weakness with or without pain and caused by injury to a collection of nerves, such as the brachial plexus
Polyneuropathies Neuropathies of several peripheral nerves simultaneously
Radiculopathies A group of disorders often caused by nerve root compression or central or neuroforaminal stenosis
Sensory nerve action potential (SNAP) The latency, amplitude, and conduction velocity recorded in sensory nerve conduction studies
Sensory nerve conduction studies Studies that test the speed by which sensory nerves transmit impulses by placing a recording and reference electrode over the nerve to be examined and then stimulating the nerve proximal or distal to the recording site
References
1. Preston DC, Shapiro BE: (eds): Electromyography and Neuromuscular Disorders: Clinical-Electrophysiologic Correlations. Boston, MA, Butterworth-Heinemann, 1998.
2. Kimura J: (ed): Electrodiagnosis in Diseases of Nerve and Muscle: Principles and Practice, ed 2. Philadelphia, PA, FA Davis, 1989.
3. Dumitru D: (ed): Electrodiagnostic Medicine. Philadelphia, PA, Hanley & Belfus, 1995.
4. Krivickas LS: Electrodiagnosis in neuromuscular diseases. Phys Med Rehabil Clin North Am 1998;9:83-114.
5. Boden SD, McCowin PR, Davis DO, et al: Abnormal magnetic-resonance scans of the cervical spine in asymptomatic subjects: A prospective investigation. J Bone Joint Surg Am 1990;72:1178-1184.
6. Haig AJ, LeBreck DB, Powley SG: Paraspinal mapping: Quantified needle electromyography of the paraspinal muscles in persons without low back pain. Spine 1995;20:715-721.
7. Preston DC, Ross MH, Kothari MJ, et al: The median-ulnar latency difference studies are comparable in mild carpal tunnel syndrome. Muscle Nerve 1994;17:1469-1471.
8. Barton NJ: Radial nerve lesions. Hand 1973;5:200-208.
9. Bradshaw DY, Shefner JM: Ulnar neuropathy at the elbow. Neurol Clin 1999;17:447-461.
10. Stewart JD: (ed): Focal Peripheral Neuropathies. New York, NY, Elsevier, 1987.
11. Strommen J: Electrodiagnosis in neuromuscular junction disorders. Phys Med Rehabil 1999;13:281-306.
12. Krivickas L, Carlson N: Myopathies. Phys Med Rehabil 1999;13:307-332.